 We deal with Glutathione in our clinic in Tulsa Functional Medicine Clinic frequently. Why? What is glutathione and what does it do?
We deal with Glutathione in our clinic in Tulsa Functional Medicine Clinic frequently. Why? What is glutathione and what does it do?
Reduced glutathione, commonly known as glutathione or GSH, is a tripeptide (3 amino acids) consisting of L-glutamine, L-cysteine, and glycine. It is ubiquitous in living systems.
Glutathione biosynthesis can be affected by biochemical individuality and/or dietary factors. Chronic oxidative stress can also deplete cellular glutathione. Precursors to glutathione, such as whey protein, vitamin C, and glutamine, are often recommended to boost glutathione levels in the body; however, results are inconsistent.
Biological individuality is such that not every body has equivalent ability to metabolize the precursors to raise glutathione.*
Glutathione has numerous cellular function benefits including antioxidant protection and detoxification. It is essential for the maintenance of cell membrane integrity in red blood cells.
Intracellular glutathione concentrations (as determined by the Spectracell test) are principally derived by intracellular synthesis, as few cells directly uptake glutathione from the surrounding extracellular fluid. The high concentration of glutathione in virtually all cells clearly indicates its importance in metabolic and oxidative detoxification processes.
Glutathione is considered the “Master Antioxidant.”
Deficiency Symptoms
A wide range of human conditions such as aging, cancer, atherosclerosis, arthritis, viral infections, AIDS, cardiovascular, neurodegenerative diseases and pulmonary diseases may be produced, or made worse, by “free radicals.”
The treatment or prevention of these conditions often includes antiooxidants such as Vitamin C, Vitamin E, carotenoids, and selenium. Glutathione is an essential component of the antioxidant defense system producing a “sparing effect” for both tocopherol and ascorbate by reducing the oxidized forms, and by eliminating hydrogen peroxide by reacting with glutathione peroxidase.
Cellular glutathione functions to decrease the formation of oxidized LDL, implicated in the development of atherosclerosis. T-lymphocytes become deficient in glutathione in the prostaglandins from n-3 and n-6 polyunsaturated fatty acids which are important in the inflammatory response.
Patients with adult respiratory distress syndrome are favorably affected by treatments that increase cellular glutathione.
Why Not Give Pure Glutathione?
Glutathione is poorly absorbed from the GI tract and foods rich in glutathione do not appear to contribute to increases in intracellular glutathione levels.
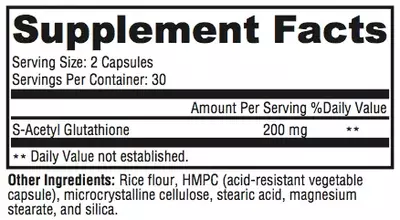
Unfortunately, most oral forms of glutathione are foul smelling, but more importantly, the majority of an oral dose is oxidized before it can be absorbed and used by the cells. This formulation delivers a unique preparation of glutathione that overcomes these usual limitations. The stability of S-acetyl glutathione through the intestinal wall and the plasma is well documented in the literature. Oral intake of S-acetyl glutathione increases total glutathione and percent-reduced glutathione. Percent-reduced glutathione is a very significant biomarker of health status.*[1-5]
Cysteine appears to be the limiting amino acid in the intracellular synthesis of glutathione and supplementation with up to 2000mg daily of N-Acetyl Cysteine appears safe.
Supplementation with normal cysteine is not recommended as it may be poorly tolerated by many patients. In addition, it may be rapidly oxidized to L-cystine, a less usable form for the synthesis of glutathione. Foods rich in cysteine are generally high protein foods such as meats, yogurt, wheat germ, and eggs.
Mechanism of Absorption
S-acetyl glutathione, a lipid-like compound, is taken up intact by chylomicrons in the gut. The acetyl bond is placed on its thiol group or sulfur group, which prevents oxidation and allows the molecule to pass diffusively into the cell after absorption in the gut.
The acetyl bond is then cleaved by non-specific enzymes inside the cell. Acetylation prevents the breakdown of glutathione, and S-acetyl glutathione does not require energy expenditure to be cleaved to reduced glutathione once it crosses the cell wall.*1-8
Antioxidant Activity
Glutathione functions extensively in tissues and organs throughout the body. It plays critical roles in protecting the body from oxidative stress, maintaining cellular functions, and supporting healthy immune function.1,4
Many factors can increase cellular exposure to oxidative insult, and therefore increase cellular consumption of nutrients—such as glutathione—that provide antioxidant activity. This may result in a fierce cycle of oxidative stress and challenges to detoxification. Complete biotransformation and protection from oxidative stress are important to maintaining cellular integrity and tissue health.*2,5
Other Benefits of Maintaining Healthy Glutathione Levels
Much information related to mitochondrial health has surfaced in the literature. Mitochondria, the energy-producing powerhouses of cells, are also the primary intracellular site of oxygen consumption and the major source of reactive oxygen species (ROS). S-acetyl glutathione has been shown to cross the membrane of the mitochondria, increasing the organelle’s activity and minimizing ROS.8,9 Reduction of ROS is associated with maintaining mitochondrial integrity and function, and improved mitochondrial health is believed to support overall health and energy.*
S-acetyl glutathione has also been shown to decrease TNF-alpha, NF-kappa beta, and F-2 isoprostane.4,9-12 Additionally, there is mounting evidence that intracellular glutathione levels in antigen-presenting cells (e.g. macrophages) may influence the Th1/Th2 cytokine response pattern and promote a balanced immune reaction.*10
Directions
Take 2 capsules daily for general support and therapy. For Alzheimer’s prophylaxis, take 1 capsule daily.
![]()
References
- Locigno R, Pincemail J, Henno A, et al. S-Acetyl-glutathione selectively induces apoptosis in human lymphoma cells through a GSH- independent mechanism. Int J Oncol. 2002 Jan;20(1):69-75. [PMID: 11743644]
- Lomaestro BM, Malone M. Glutathione in health and disease: pharmacotherapeutic issues. Ann Pharmacother. 1995 Dec;29(12):1263-73. [PMID: 8672832]
- Cacciatore I, Cornacchia C, Pinnen F, et al. Prodrug approach for increasing cellular glutathione levels. Molecules. 2010 Mar 3;15(3):1242- 64. [PMID: 20335977]
- Vogel J, Cinatl J, Dauletbaev N, et al. Effects of S-acetylglutathione in cell and animal model of herpes simplex virus type 1 infection. Med Microbiol Immunol. 2005 Jan;194(1-2):55-59. [PMID: 14624358]
- Ballatori N, Krance SM, Notenboom S, et al. Glutathione dysregulation and the etiology and progression of human diseases. Biol Chem. 2009 Mar;390(3):191-214. [PMID: 19166318]
- Richman PG, Meister A. Regulation of gamma-glutamyl-cysteine synthetase by nonallosteric feedback inhibition by glutathione. J Biol Chem. 1975 Feb 25;250(4):1422-26. [PMID: 1112810]
- Anderson ME, Powrie F, Puri RN, et al. Glutathione monoethyl ester: preparation, uptake by tissues, and conversion to glutathione. Arch Biochem Biophys. 1985 Jun;239(2):538-48. [PMID: 4004275]
- Anderson ME, Nilsson M, Sims NR. Glutathione monoethyl ester prevents mitochondrial glutathione depletion during focal cerebral ischemia. Neurochem Int. 2004 Feb;44(3):153-59. [PMID: 14568558]
- Kretzschmar M. Regulation of hepatic glutathione metabolism and its role in hepatotoxicity. Exp Toxicol Pathol. 1996 Jul;48(5):439-46. [PMID: 8765689]
- Fraternale A, Paoletti MF, Casabianca A, et al. Antiviral and immunomodulatory properties of new pro-glutathione (GSH) molecules. Curr Med Chem. 2006;13(15):1749-55. [PMID: 16787218]
- Kretzschmar M, Klinger W. The hepatic glutathione system—influences of xenobiotics. Exp Pathol. 1990;38(3):145-64. [PMID: 2192911]
- Donnerstag B, Ohlenschlager G, Cinatl J, et al. Reduced glutathione and S-acetylglutathione as selective apoptosis-inducing agents in cancer therapy. Cancer Lett. 1996 Dec;110(1-2):63-70. [PMID: 9018082]